Dr. Pawluk regularly reviews literature on magnetic technologies and treatments. Below, we have listed some excerpts from a range of publications and articles we believe to be interesting and thorough, and which show support for the basic concepts of the healing effects of magnetic field therapy. Some are Dr. Pawluk’s own publications.
Harvard Medical School, Boston, MA, Medical University of Vienna; 2009 March
“In conclusion, our study provides evidence for a beneficial effect of PEMF on scores in general and ADL in specific for patients with OA of the knee. Our results showed no significant effect on pain, but left enough space for improvement to significant values in forthcoming, larger studies (28). These findings suggest that PEMF might be a useful and effective addition to the conservative management of OA of the knee. Future studies are needed to prove this assumption right or wrong.”
Tenforde TS. Bioelectromagnetics; 2003 Jan;24(1):3-11
In this acceptance address for the Bioelectromagnetics Society’s 2001 d’Arsonval Award, Dr. Tenforde reviews the highlights of the nonionizing field aspects of his research and scientific service career. These are focused in four areas:
(a) development and application of microelectrophoretic methods to probe the surface chemistry of normal and cancerous cells; (b) research on the biophysical mechanisms of interaction and the dosimetry of static and extremely low frequency magnetic fields; (c) application of extremely high intensity magnetic fields in several spectroscopic methods for probing the detailed structures of large biological macromolecules; and (d) development of national and international guidelines for the exposure of workers and members of the general public to electromagnetic fields with frequencies spanning the entire nonionizing electromagnetic spectrum.
Furthermore, Dr. Tenforde’s pioneering work in the field of nonionizing electromagnetic radiation has undoubtedly had a significant impact on our understanding of these phenomena. His research, consequently, has led to a deeper appreciation of the potential effects of electromagnetic fields on biological systems and the importance of establishing guidelines to ensure the safety of workers and the general public.
Additionally, his contributions in areas such as microelectrophoresis, dosimetry, and high-intensity magnetic fields have marked a distinctive path in the scientific community. Moreover, the application of his findings to cancer research and the study of biological macromolecules underscores the breadth and significance of his work.
In summary, Dr. Tenforde’s multifaceted career underscores the indeed critical role of interdisciplinary research and international collaboration in advancing our knowledge of nonionizing electromagnetic fields. His work has provided undeniably valuable insights into the complex interplay between electromagnetic radiation and biological systems.
Rubin CT, McLeod KJ, Lanyon LE. J Bone Joint Surg Am; 1989 Mar;71(3):411-7
Using an animal model, we examined the use of pulsed electromagnetic fields, induced at a physiological frequency and intensity, to prevent the osteoporosis that is concomitant with disuse. By protecting the left ulnae of turkeys from functional loading, we noted a loss of bone of 13.0 per cent compared with the intact contralateral control ulnae over an eight-week experimental period. During using a treatment regimen of one hour per day of pulsed electromagnetic fields, we observed an osteogenic dose-response to induced electrical power, with a maximum osteogenic effect between 0.01 and 0.04 tesla per second. Pulse power levels of more or less than these levels were less effective.
The maximum osteogenic response was obtained by a decrease in the level of intracortical remodeling, inhibition of endosteal resorption, and stimulation of both periosteal and endosteal new-bone formation. Moreover, these data suggest that short daily periods of exposure to appropriate electromagnetic fields can beneficially influence the behavior of the cell populations that are responsible for bone-remodeling, and that there is an effective window of induced electrical power in which bone mass can be controlled in the absence of mechanical loading.
Levin M. Bioelectromagnetics; 2003 Jul;24(5):295-315
Understanding the factors that allow biological systems to reliably self-assemble consistent, highly complex, four-dimensional patterns on many scales is crucial for the biomedicine of cancer, regeneration, and birth defects. The role of chemical signaling factors in controlling embryonic morphogenesis has been a central focus in modern developmental biology. Additionally, while the role of tensile forces is also beginning to be appreciated, another major aspect of physics remains largely neglected by molecular embryology: electromagnetic fields and radiations.
The continued progress of molecular approaches to understanding biological form and function in the post-genome era now requires the merging of genetics with the functional understanding of biophysics and physiology in vivo. Furthermore, the literature contains much data hinting at an important role for bioelectromagnetic phenomena as a mediator of morphogenetic information in many contexts relevant to embryonic development. This review attempts to concurrently highlight briefly some of the most promising (and often underappreciated) findings that are of high relevance for understanding the biophysical factors mediating morphogenetic signals in biological systems. These data originate from contexts including embryonic development, neoplasm, and regeneration.
William Pawluk, MD, MSc; 2002 December
There are many approaches to preventing and managing stress reactions. Once a stress reaction is initiated, it is difficult to turn off immediately. The reaction is immediate, but the recovery takes hours to days. Nonetheless, since the effects of stress are cumulative, a daily routine of reducing the physiologic response becomes necessary to ward off long-term damage. Moreover, one approach to reducing the physiologic response to the effects of daily stress is whole-body pulsed magnetic field (PEMF) therapy.
Furthermore, the use of PEMF therapy is gaining recognition as an effective means of addressing stress-related issues. Additionally, it can be a valuable tool in managing stress reactions, as it offers a noninvasive and drug-free approach to mitigating the consequently harmful effects of stress on the body.
Henceforth, individuals who incorporate PEMF therapy into their daily routines can experience the benefits of reduced stress reactions and enhanced overall well-being. Therefore, it is important to explore various stress management techniques and find the one that works best for you.
William Pawluk, MD, MSc: 2003 March
Pain patients with lumbar radiculopathy or whiplash syndrome had a PEMF applied twice a day for two weeks and their pain medications decreased. Radiculopathy pain relief happened in 8 days in the PEMF group vs 12 days in the controls. Headache pain was halved in the PEMF group and one third less of neck and shoulder/arm pain vs control.
An Interview with William Pawluk, MD, MSc
Russ Mason, MS: Alternative and Complementary Therapies Journal, Vol. 8, No. 2, April 2002
Dr. Pawluk’s exploration of a broad range of healing modalities led to his major interest in using magnets and electromagnetic energy to support the healing and written process… In this interview, Dr. Pawluk describes the winding course of his life’s work, and his interest in energy medicine–including medical uses of magnetism–with author Russ Mason.
An important new study shows that seizures may be inhibited by the prior use of low frequency, low intensity PEMFs.
Mice were injected with an agent that almost always induces seizures. There were several groups. One did not get PEMF exposure to serve as a control. Others were exposed 2 hrs per day for different duration’s of the PEMF prior to injection. This was for 1 day, 3 days, 2 weeks, or 1 month. The dose of agent needed to induce seizures was determined. All exposures produced benefit, but the longest duration of exposure produced the strongest, most significant protection, with the amount of protection increasing with the duration of exposure. Seizures were induced in all PEMF unexposed mice. This study indicates that long term PEMF use at or around 2 hours per day will provide the greatest protection at the PEMF intensity and frequency used.
It is not known whether stronger PEMFs will exert more protection. It’s also unknown whether longer exposure times per day will be better. It is also not established whether these results can be expected in humans, but the results provide very strong support that these types of PEMFs could be considered to be effective even in humans. This type of research cannot ethically be conducted in humans, so it may never be known for certain, except that other approaches to studying this possibility could be considered. At the very least, the results provide support for reducing concern that these types of PEMFs may initiate seizures.
Since seizures in humans are somewhat unpredictable as to when they may occur, use of PEMFs would likely be needed to be used long term, if not lifelong. Since animals are typically more sensitive to PEMFs than humans, these PEMFs may even be useful in children, particularly when seizure activity is frequent and poorly controlled by medication. The situation of intractable seizures is a fairly common and frustrating health and management problem.
This study points out that longer treatment times are likely needed than most PEMF systems can deliver without some inconvenience. So, if someone were to consider using PEMFs for managing seizures, they would need a system that can be applied for extended times.
I cannot advise that PEMFs should be relied on as a sole therapy for seizures, except in the circumstance of medication intolerance or poor control with available medications. Seizures have many causes, so results may be unpredictable depending on the cause. This study did not address different forms of seizures. Ultimately, individual experience will have to guide how this form of therapy would be able to be used.
It could also be expected that PEMFs used along with medication may allow medication dosing to be reduced. Thus, reducing risk of side effects. In almost no circumstance could I advise stopping seizure medications prior to knowing how effective the PEMF therapy would be.
Fadakar K, Saba V, Farzampour S. Acta Neurol Belg. 2013 Jun;113(2):173-7. Effects of extremely low frequency electromagnetic field (50 Hz) on pentylenetetrazol-induced seizures in mice.
Scleroderma or progressive systemic sclerosis (PSS) is a very complex condition, with a major autoimmune component. Food allergies need to be ruled out as a potential cause. Pulsed electromagnetic fields (PEMFs) may be effective for controlling certain aspects of scleroderma. However, it would not be expected to cure or turn off the condition. Basically, PEMFs would be very helpful to control some of the complications and side effects of the scleroderma. It may actually slow down its progression. There is no reason that it could not be used alongside any other therapies, including disease modifying regimens. I was able to find two studies that evaluated its use. I have no testimonial experience treating this condition.
The first study comes from my book. 20 scleroderma patients with Raynaud’s syndrome were treated with a PEMF applied to the spine at C4-Th7 and Th10-L2 vertebrae. They found that 95% had improvement in excess of palmar sweating, cold sensitivity, reflexes and ulnar nerve conduction. Velocities increased by 5-7m/s.
The second controlled clinical trial looked at treatment with a different PEMF in combination with other conventional and alternative therapies, which included physical therapy, supplements, and massage. This study had 80 patients, 52 of whom had local thickening/induration and 28 head multiple areas involved. The study had a basic group and a comparison group, with 40 in each, and a third control group of healthy people. The therapy group had the usual therapies plus PEMFs, whereas the control group only had the usual therapies.
Treatments were applied every other day for a course of 12 procedures. They were evaluated using clinical and immunological testing. The treatment group had full recovery in 16 of 40 individuals, with significant improvement in another 22 (95% showing at least some improvement). The control group had full recovery in only 10 and significant improvement in 19 (73% showing at least some improvement). There was a highly statistically significant improvement in immune indices compared to the control group, including immunoglobulins, blast transforming activity of lymphocytes and complement. They concluded that PEMFs facilitate clinical as well as immunological improvements in scleroderma/PSS.
While these studies indicate benefit in scleroderma patients with even a limited course of use, it would be expected that continuing benefit would be seen with continued use over the long-term. It may be necessary to continue traditional disease modifying agents (DMARD treatments) at the beginning, depending on the severity of the scleroderma, and then gradually taper them off with continued PEMF use and monitoring of clinical parameters. Adding oral type I collagen supplementation to the treatment protocol may also add to the benefit of PEMF’s to improve the thickening of the tissues, since PEMFs, have been found to improve scars caused by aggressive collagen deposition.
I am now reminded every day that I am in my 60s. My body reminds me from multiple locations. While I’m not a professional or even a semiprofessional athlete, I have accumulated numerous aches and pains as a weekend warrior over the years.
My first significant injury occurred while playing sandlot football in my final year of medical school. I jumped up to snare a pass and was turning around as my leg was planting. It felt an immediate pain in my right knee and limped off the field. Within minutes, my knee was as big as the football. Several hours later my knee was tapped, producing frank blood. That was in 1970. Orthopedics was still relatively primitive at that time. The surgical option was certainly more potentially debilitating than learning to live with the injury. It was a torn menisci and a complete ACL rupture. That injury limited the aggressiveness of any sports I would engage in for the rest of my life. This included tennis, downhill skiing, racquetball, etc.
However, I did play a little bit of softball. I practiced pitching and catching with my kids as they were growing up, and some soccer practice. The limitations I had to endure were fairly acceptable to me. This was because I got wrapped up in my medical career, which basically consumed most of my time.
My daughter tore her ACL playing college field hockey. After she had a successful ACL repair, I decided to see an orthopedic surgeon regarding my options. His examination showed that I had a completely ACL-deficient knee. I didn’t need to worry about the menisci catching or locking–my knee was that loose. He said that I was lucky in that I had a small frame and was not greatly overweight. Otherwise, I would have had to have had a procedure long before. At that point I elected not to do surgery since I couldn’t afford the downtime. The only thing that I must do now to compensate is to wear a knee brace for my morning 3-mile walks.
Instead of spending a good part of my free time in various sports activities, I directed my energies into learning. This included healing arts outside the typical medical paradigm. I discovered and became trained in acupuncture through a UCLA program for physicians. After that, I learned a lot about energy medicine and how far ahead of us the Eastern Europeans were. They had discovered the marvelous effects of pulsed electro-magnetic fields (PEMFs) decades earlier.
I am daily in need of treatments for my various aches and pains, as a weekend warrior. But I am no longer tied to only one discipline or approach to achieve results. Most commonly, relying on PEMF therapies. Only my own PEMF system has given me the liberty and flexibility to treat myself as I need, day in, day out.
I have been working with Dick Butkus regarding his own “weekend warrior” state. He spent plenty of time playing professional football. He clearly has more “wounds,” that is, aches and pains and limitations, than I do. This is not unexpected.
As happens with most Americans in this situation, he has accessed all the usual approaches to his health issues. This is with some but not complete benefit. The one therapeutic approach most athletes and Americans have never heard of is the use of PEMFs. This issue was recognized by Dr. Oz when I appeared on his show. The American healthcare community is only just beginning to wake up to the potential offered by PEMFs. I am aware of quite a number of athletes who are already using this technology. There is a range of results. Because there are a large variety of PEMF devices promoted, the challenge is finding the right device for the specific individual’s needs.
The classical approaches include medical management, physical therapy, chiropractic, sports medicine, acupuncture, massage and others. The major challenge for most people with all these classical approaches is that you need to continue to see a practitioner to receive services. Sometimes, all that is achieved is temporary improvement or benefit. With an acute injury, usual approaches work quite well to shorten the time of healing.
Unfortunately, acute injuries frequently convert to chronic problems. This is where the problems really begin. What if there is a technology available that allows you to treat yourself at your own convenience? In your own home setting or as you are out and about during the day? In addition, what if this technology is very safe, non-toxic, noninvasive and not that expensive? Wouldn’t that be of interest to you? Unfortunately, again, most commonly, your practitioners are not going to recommend this to you.
There are several reasons. As Dr. Oz mentioned, most practitioners are not even aware of this technology. Unfortunately, I have discovered that even when we try to provide them the information to have them become aware, they may be resistant to recommending it for intellectual, professional, administrative, legal or financial reasons. Most clinicians are comfortable with what they know and do, and rarely reach outside their comfort zone, especially when a therapeutic approach is not supported by their professional community or the “establishment” in general.
Most of the time, it’s about the doctor getting through his/her day. It’s not about “what am I missing here?” or “is there something else I can do to help this person, since what we are doing isn’t working?“ Clearly, it’s not always this way. There are many open-minded – and humble – doctors who really want to help the person but are stuck in a mental “rigid cage” they can’t break out of. I had to do that, to break out of my own and my colleague’s cages. I took a course in medical acupuncture, and it changed my view of other options to help my patients, outside the medical toolbox.
Today, I wish I could say that even your usual medical doctor would refer you to nonconventional practitioners without you having to ask for the referral. But conventional medical doctors tend to have blinders on relative to other types of non-medical practitioners. The reason is that they don’t understand what these other practitioners do. The medical journals don’t help, because they never publish information about how to live in a cooperative community of willing practitioners. Also, they tend to look down on nonconventional practitioners because they are not “doctors.” Of course, this situation varies from doctor to doctor and, also, around the country. Many professions fall into these same traps. Professional team trainers and doctors also frequently fall into this mode. Usually, it’s on the athlete and/or person himself or herself to take the initiative to “vote with their feet” or ask for a recommendation.
Pain medications can be addicting, create all kinds of side effects, and even cause death. One of the most commonly used medication groups are nonsteroidal anti-inflammatory drugs (NSAIDs). NSAIDs have been found to cause about 16,000 deaths per year due to gastrointestinal hemorrhage. In addition, NSAIDs damage the kidneys and liver. Chronic dependence on NSAIDs reduces the body’s capacity to heal itself from injury. Acetaminophen including Tylenol) damage the liver. Thousands of people a year end up with liver failure due to acetaminophen overuse. Narcotics such as codeine, oxycodone, and OxyContin are addicting. Their use escalates during the addiction process and there is a significant illegal market in these drugs. Thousands of people die per year from overuse, abuse and side effects from narcotics.
There is an even more insidious problem with all these medications and drugs: they end up in the urine of the users, which ends up in groundwater, which ends up in our water supply. Therefore, we are all (including our children and pregnant women) involuntarily taking these pain medications into our bodies. Objective research studies found these substances showing up in our water supply in major urban areas, since there are so many people using these drugs now.
Injections create their own problems. Most injections use steroids. We have all heard about the recent spate of fungal meningitis deaths caused by epidural steroid injections. Local injection of steroids creates its own tissue destruction, leading ultimately to an increased risk of injury and further damage to the surrounding tissues. A person is usually limited to 1 or 2 injections into the same location in a lifetime because of these risks. At the most, injections give only temporary relief. Because of the physical stress the athlete undergoes–the breakdown of ligaments, tendons and muscles–the athlete is at even further risk of future injury. Unfortunately, the decision is driven by the moment at hand, and not with any consideration for future risk.
Procedures and surgeries can be dramatic and can help the athlete get back into competition, but the results are very unpredictable and often lead to major complications that become permanent and potentially even more disabling. The problem with surgery is that no one can ever tell where the actual pain generator is in the tissue. So, it is common that the procedures do not result in any benefit, or if there is a benefit, it is short-lived before the pain returns.
Because of our dependence on insurance coverage for medications and other medical therapies, people often do not avail themselves enough of alternative approaches, particularly for chronic pain.
There are many. A short list includes: chiropractic, massage, acupuncture, physical therapy, dietary changes, herbs and supplements, mind-body approaches, healing techniques such as Reiki, and energy medicine technologies.
I have been trained in acupuncture, nutrition, mind-body techniques and energy medicine. I have used all these approaches with differing success. When I did my training in acupuncture in 1990, it was very early in its acceptance in the US and was mostly shunned. So, at that time I started looking for alternatives to using acupuncture and came upon the use of magnets.
Magnets have been used in the Orient for decades, even centuries, to stimulate acupuncture points, as an alternative to using needles. As I started delving into the science behind magnetics and its effects on biology, I realized there was a large body of literature to support positive effects in the body. I also began to see that a lot of the science had to do with electromagnetic therapy and not physical magnets. Physical magnets are often called static magnets because, once they are formed, they remain magnetic. In other words, the magnetic field is not turned on or off, but remains constantly the same.
Because there was so much more science behind electromagnetic therapy, I eventually met up with a MD-PhD doctor from the Czech Republic who had translated much of the Eastern European science behind the use of medical magnetic fields. As a result, we collaborated and published a book, Magnetic Therapy in Eastern Europe: a Review of 30 Years of Research. Now, this is not a book for the average person-it is very technical. Nevertheless, the point here is that there was a decent amount of experience already using PEMFs to treat various medical conditions, most commonly pain.
After this, a large amount of my personal clinical effort towards managing pain clinically shifted to using PEMFs.
The big advantage is that PEMFs do no harm and they do a much better job at impacting the causes of pain.
The causes of chronic pain include swelling in the damaged or injured tissue, lack of circulation, inflammation, poor ability to regenerate damaged tissue, nerve damage, muscle spasm, and others. Certainly, cutting oneself, burning oneself, having an infection destroying tissue, are all causes of pain. These types of injuries often resolve on their own given enough time. But for those with chronic pain, these acute problems often convert into chronic problems because they just don’t heal themselves properly.
A lot of chronic pain, such as arthritis or pain caused by a bulging disk in the lower back, is not due to any obvious cause. Chronic pain is often associated with aging. I describe aging as “death by 1000 cuts”. So, aging and chronic pain are often caused by a lifetime of many minor injuries. This is seen most commonly in professional athletes, who endure multiple injuries over their professional and personal playing time.
Pulsing magnetic fields go right through the body as if the body was not even there. It can be visualized as wind blowing in the trees. You can’t see the wind, but you can tell it’s there because the leaves are rustling. The wind does not stay in the tree, but just passes on through. So do pulsed magnetic fields. While they are passing through, they stimulate the cells of the body and produce increased energy in the tissues, shifting many chemical processes. The increased energy can then be used by damaged or injured cells and tissues to repair themselves. This is a self healing process.
This was a point made by Dr. Oz : pulsed magnetic fields can be a cure for pain. PEMFs treat the cause of the pain, not just the pain itself. They are not a Band-Aid, although they can act that way sometimes, too.
Magnetic fields have been found to have a pain-killing effect equal to about 10 mg of morphine, so not only do they help resolve the underlying cause of the pain problem, but they also can help to produce a natural pain-reducing effect.
The Internet is full of information on magnets and magnetic therapy. There are many pulsed electromagnetic field devices sold on the Internet as well. The information is very confusing, and people often make significant claims that their machines or devices are the best.
I have set up a website, DrPawluk.com to provide more scientifically- and medically valid information about pulsed electromagnetic fields. As a physician, it is my ethical obligation to provide people with choices. The more research I did and the more devices I reviewed and used both in my practice and for myself and my family, the more I realized there is no one size that fits all and there is no one device that is a perfect solution for all problems.
As a result, I have presented reviews of several different devices that I have used and recommended. As I said, I do not typically emphasize any one device over any other. The choice of the device for anybody with chronic pain will depend completely on the nature of the pain they have. Certainly, some devices are better for certain kinds of problems than others. I will therefore use certain devices for more specific situations. Part of the question about which device to use depends on whether the problem is local or general, or whether there is more than 1 location of pain, which is often the case. Another option is whether the device is portable or requires you to be in one place for extended periods of time to get your treatment.
A major block for most people in using PEMFs is the need to plug them into an electrical outlet. This limits flexibility and the ability to continue once daily activities. It is for this reason that I often will recommend the FlexPulse device.
One of the FlexPulse signals was originally developed for NASA to stimulate stem cells. It was subsequently found to dramatically enhance bone healing, including after major bone surgery. Most recently, it has been found to reduce acute inflammation at least 50% as well as steroid injections – although obviously without all the side effects and potential risks. Not to mention that when you own one of these devices you get use it for the rest of your life, as opposed to a single injection which only works temporarily.
Anybody who wishes to reduce their chronic aches or pains without relying on medications, who wants to avoid injections, procedures or surgery, who had all these procedures, and they didn’t work or developed complications or anybody who simply is looking for an alternative approach to manage their pain. PEMF therapies can be used alongside most other therapeutic modalities. In fact, combinations of approaches are often even more effective. Who wouldn’t want at least a 30 to 70% reduction in their pain, if not even elimination of it?
I often tell people the following when they already own a pulsed electric field therapy system. They don’t own it, the house owns it. This includes the dog, the cat and the plants. PEMFs are just as effective-often even more effective-in animals than they are in people. In fact, much of the research on PEMF therapies has been done in animals, so the results certainly have been proven.
Where can I find more information about PEMFs?
I offer the websites, DrPawluk.com and FlexPulse.com as places and the book “Power Tools for Health”. You can find credible, scientifically based information and education about pulsed electromagnetic field therapies. I also provide reviews of different PEMF products that give you options of different approaches using pulsed electromagnetic field therapy. These reviews help to reduce confusion about the different devices, objectively and with balance. Furthermore, there is a PEMF Buyer’s Guide on DrPawluk.com about how to make decisions as to which PEMF system is best for you.
William Pawluk, MD, MSc
The pain associated with shingles (herpes zoster – HZ) is one of the most intolerable pains people have to endure. And, about 1 out of 5 people, after a shingles attack, will experience a worse, persisting, and debilitating pain called postherpetic neuralgia (PHN). The pain can get better after a few months, though in some people it will last even longer. Doctors don’t know why shingles converts into PHN. PHN is considered neuropathic pain or a form of neuropathy.
One million shingles attacks occur every year in the US, and one in every three people develops shingles during their lifetime. The shingles virus (called the varicella zoster virus or VZV) is the same virus as the chickenpox virus. The first infection with the virus (the primary infection) is chickenpox, typically occurring in children. Shingles (a secondary condition) is a consequence of the first infection, chickenpox. Prior to the use of childhood vaccines in the U.S., more than 90% of Americans had chickenpox before the age of 20. After a chickenpox infection heals and immunity develops, the virus becomes dormant, and lives and persists in a cluster of nerve cells (a ganglion) in a spinal nerve anywhere along the spine.
A shingles outbreak develops when the dormant chickenpox virus is reactivated in the spinal nerve roots, then migrates to the nearby related sensory nerves, causing a rash along that sensory nerve’s pattern (dermatome). Most commonly the rashes occur on either the head, face, chest or torso. The course of shingles and pain is usually one-sided and follows the affected sensory nerve pattern (dermatome) on that side. Because the dormant virus is normally suppressed by the immune system, reactivation only occurs in people whose immunity is weakened, whether temporarily, or as a factor of age. Psychological stress, or a dramatic life event may contribute to shingles flare-ups. People can have multiple shingles attacks in a lifetime.
20% of people aged 60–65 years will develop PHN, and more than 30% of those over 80 years will develop it. In addition to age, risk factors for developing PHN after shingles are based on the way the shingles attack shows itself:
By way of example, an elderly woman with severe pain and a sudden onset rash has a greater than 50% chance of developing PHN, whereas her risk is only 10% when none of these factors is present.
In the first stages of the shingles attack, pain is typically moderate to severe. Those suffering from a shingles attack have ranked the pain as more intense than post-surgery, or labor pains. However, PHN can develop into chronic pain, which can seriously affect a person’s ability to continue regular activities. This pain can become relentless and can persist for months or even years after the acute disease phase. In one study of people over 65 years old with PHN, the average length of pain was 3 years, and ranged from 3 months to more than 10 years.
Those with PHN experience three major types of pain, lasting for at least 3 months after healing of the skin rash caused by shingles:
1) constant burning, aching, or throbbing pain,
2) intermittent stabbing, shooting, or electric shock-like pain, that can happen without a stimulus, and
3) pain brought on by a stimulus, such as a light touch, but not proportional to the stimulus (exaggerated pain).
Additionally, those with PHN have reported other abnormal sensations in the skin. These have been described as itchy, burning, restrictive, numbness or feelings of pins-and-needles. Those with PHN have reported a severely decreased quality of life due to interference with daily activities and functions, decrease in physical ability, and the psychological toll it can take. As a result, PHN is usually accompanied by anxiety, depression, and dissatisfaction or frustration in being able to fulfill hopes or expectations.
Shingles attacks are frequently treated with antiviral medications. These medications do not kill the virus, but instead limit its growth so that the attack may be less severe. A more effective strategy may be to get shingles immunizations; though even these do not prevent future shingles attacks, but may limit the likelihood or degree of PHN. In other words, they are not foolproof.
Once it develops, there is no cure for PHN. Controlling pain is the primary treatment strategy. Medication and nerve destruction are the most common therapies in medical practice. Pregabalin and gabapentin, the two most widely used drugs, are often only slightly helpful. A survey conducted in 2002 of 385 patients aged 65 years or older with persistent PHN who were receiving prescription medication, found that only 14% were highly satisfied with their treatment (Bonezzi). Although these therapies can partially relieve the pain, they may cause undesirable side effects and high risks of complications. Therefore, therapies that can relieve neuropathic pain safely and noninvasively without causing severe side effects are desperately needed.
Pulsed magnetic field device (PEMF) therapy was recently studied to see if it would be beneficial to those suffering with PHN. PEMF device therapy is painless and noninvasive. Because PEMFs cross through the brain, the form of PEMF therapy used in the study was applied to the skull; this is called transcranial magnetic stimulation (TMS). TMS has a painkilling analgesic effect level similar to a surgically placed, epidural electrical stimulation implant. It is dissimilar, however, to the electrical stimulation implants, in that TMS does not have a high risk of failure and complications. Additionally, TMS device-type magnetic fields can also be used to stimulate peripheral nerves and muscles.
Because it is painless and noninvasive, TMS is considered one of the most important brain technologies of the 21st century. TMS is being widely applied in clinical psychiatry, for neurologic disorders, and in rehabilitation. Studies have proven that TMS is effective in improving pain, sleep quality, and anxiety of patients with PHN.
One study (Pei) evaluated the use of TMS for PHN. In this study, 3 treatment schemes were used, equipment placed over the head but not actively stimulated (sham), TMS at 5 pulses per second [PPS], and 10 PPS. The effectiveness and safety of these treatments were compared to see which treatment scheme might be best.
Methods: Sixty patients with PHN were divided into 3 equal groups. TMS was applied with a coil to the side of the head just above and behind the ear (over the primary motor cortex – M1) on the healthy side of the body. Active stimulation was at an intensity of 80%, once daily for 10 days. For the 5-PPS group, each session included 300 one-second pulses at 5 PPS for a total of 1500 pulses per session.
For the 10-PPS group, each session had 300, 0.5-second pulses, for 1500 pulses per session. In all groups, total session time was 17.5 minutes. All had conventional medication therapy. Everyone received evaluations at different time points (before treatment (T0); 10 times during treatment (T1-T10); 1 month after treatment (T11); and 3 months after treatment (T12). Evaluations were for level of pain (VAS), quality of life (QOL), sleep quality (SQ), depression (SDS), and impression of change (PGIC), and incidence of adverse events.
Results: Compared with the sham TMS group, there was a significant reduction in pain scores in the active treatment groups at T2-T12. Pain scores in the 10 PPS TMS group at T7-T12 were significantly better than the 5 PPS group. The average pain score reduction was 28% with 5 PPS TMS compared to 40% with 10 PPS TMS. The quality of life, sleep and impression of change scores of both the active treatment groups at 3 months (T12) after the treatments ended were significantly better than the sham group. This indicated that there were long-term benefits from PEMF device TMS treatment, including in quality of life and sleep quality.
Pain score reduction in the 5 PPS group was not as good as the 10 PPS group. The same was true for quality of life and sleep scores. This is presumed to be because 10 PPS may be more alerting to the brain through the entrainment effect of more rapid, alpha frequency pulses.
As is usual with PEMF studies, adverse events among the 3 groups after TMS were not significant.
Other research (Ma) also found that PEMF device treatment with TMS was safe and effective. Mean pain scale (VAS) reduction in the real TMS group was 17% for people who had PHN longer than 6 months. VAS was significantly reduced by 100% compared to sham for the real TMS group along the whole time-course of the study. No significant daily pain level changes were seen for sham TMS. For those whose pain scores before starting PEMF device TMS treatment were greater than 7 of 10, the reduction in pain was 52% compared to a 30% reduction in those whose scores were less than 7. These pain reduction and analgesic benefits were followed by long-term improvement in quality of life. Reduction in need for medications at week 5 was significantly better in the active TMS magnetic device group than in the sham group.
In the real PEMF device TMS treatment group, six patients reported minor adverse events with four reports of neck pain and headache, and two reports of dizziness and dry mouth. These did not require a change in treatment. Of the 20 patients from the sham TMS group, four also complained of neck pain and headache, and one complained of dizziness. Essentially there was no difference. So, it’s unlikely that TMS treatment was the cause of the symptoms.
It may seem counterintuitive to treat the brain for chronic pain, whatever the cause, when the pain is caused by a problem, or felt elsewhere in the body. Too often, people treat where they feel the pain but not the source of the pain. Treating the actual area of the pain, where the blisters were, is less likely to produce significant benefits.
The source of the pain in PHN is coming from the nerve roots at the level of the spine from which the shingles pain signal starts. At the very least treatment needs to be to the spine at the level where the nerves are affected. These two brain PEMF device stimulation studies seem to indicate a major improvement in pain. However, sleep, and quality of life in people with chronic, long-lasting PHN, these benefits were not from treating the specific areas generating the pain or the areas where the pain was felt.
This brain transcranial magnetic stimulation (TMS) research used a different approach. It recognized the need to treat the brain itself, which is the “last stop of the train” of the pain signal.
PHN is commonly severe, disabling, and potentially very chronic. I normally recommend using higher intensity PEMF device treatments to deal with this type of pain. Based on the TMS research, magnetic field intensities needed to treat the brain adequately are over 5000 Gauss [500 mT]. It’s possible that lower magnetic field intensities may be useful to treat the nerve roots. More information about the level of the magnetic field needed to treat the cause of the pain, that is, inflammation, can be found here.
For the most dramatic PEMF device PHN pain-reducing results, I would recommend a combined 3 level approach.
It would be best to have a PEMF system with at least 2000 gauss and preferably closer to 4000 Gauss. These intensities are still less than the scientifically studied PEMF device TMS systems. These are around or above 5000 Gauss.
The other important thing to consider is that PHN can be chronic and will likely require ongoing treatments. The length of time treatments will be needed is entirely individual. In both the studies I mentioned above, people received daily treatment for 10 days. Even though pain was reduced by 28-40%, it was not relieved completely. It is not known yet whether treatment beyond 10 days would produce even better results. My clinical experience is that longer courses of treatment are needed for the best results.
Also, the Pei study showed that pain continued to decrease from a level of 6.3 out of 10 to 4.3. This was true as long as treatment continued over the 10 days. Even at that lowest level (4.3), that is still a significant amount of pain, and would dramatically affect the quality of life. The goal should be to try to reduce the pain to 0 if possible.
Another consideration is that this research was limited to people who already had established (PHN) and was not done at the time of the initial shingles attack. The sooner treatment begins after a shingles attack starts, the better and more long-term the results will be. Ideally, treatment should begin at the first sign of shingles. This will not only help to reduce the pain of the shingles during an attack, but will also help to reduce the likelihood of the shingles developing into PHN.
If a person waits to start PEMF device treatment after PHN has developed, it will be much more difficult to reverse the problem. The longer treatment is delayed after shingles starts, the more the nerve inflammation and infection can progress. This leads to more and more nerve damage (neuropathy) and pain. Unfortunately, antiviral medications do not kill the viruses that cause shingles and PHN. All they do is to stop the virus from reproducing even more. Nevertheless, they are still useful. And pain medications do nothing to stop the progression of the damage. They don’t limit the attack and will not reverse it or reverse the nerve damage. In fact, some research shows that pain medications may significantly inhibit natural anti-viral white cells. These are called natural killer (NK) cells, which attack and destroy viruses.
So, it makes a lot of sense to combine PEMF device treatments with antivirals and NK cell activator supplements. This controls the shingles and subsequent PHN.
PEMF device therapy can be extraordinarily useful with shingles attacks. They can be used used until after postherpetic neuralgia (PHN) starts. They can still be very helpful to decrease pain levels and improve quality of life. Getting and using the right intensity magnetic field becomes critical to getting the right level of benefit. Following a 3 level PEMF device treatment approach should give the best results for this serious and disabling PHN condition.
There is much press recently about the use of FDA approval. This involves high intensity, prescription level, repetitive/rapid transcranial magnetic field (rTMS) stimulation. It is for the treatment of psychiatric and neurological conditions. PEMF therapy for brain and neurological conditions has greatly increased curiosity in the recent years. These devices certainly do have significant benefits in many of these neurological conditions. At this point they require prescription by doctors and have limited coverage by insurance. A course of treatments is usually 10-20 sessions and costs upwards of $200 per treatment.
At this time there are very few facilities or physicians that offer these treatments. One example of an FDA approved system is the NeuroStar. The cost to place a system into a doctor’s office is about $50,000, as last we heard. The question becomes can other PEMF therapies produce comparable or similar results to these high-intensity PEMF devices? Other systems, comparable to the North Star, have been approved in other countries, including Canada.
It is necessary to say that other devices of lower intensity and different applicator configurations have not been compared head-to-head with these high-intensity rTMS systems. There is evidence to suggest that even extremely tiny intensity magnetic fields [pico Tesla] have shown benefit in a wide range of neurological and psychiatric conditions. Research also shows that less powerful PEMFs can have significant effects on EEG brainwave patterns.
Changes in EEG patterns definitely affect neurochemistry and therefore mood. Controlling the intensity of PEMFs (especially to achieve lower intensities) may be important for many people. In addition, rTMS rarely achieves frequencies higher than about 20 Hz. It is known that many inflammatory regenerative processes require higher frequencies. There can be significant side effects from the use of rTMS. This is true even in well-controlled settings. Therefore, lower intensity PEMFs may have a role and place in helping individuals with many conditions for which rTMS has been applied.
I wrote a book on magnetic therapy, Magnetic therapy in Eastern Europe: a review of 30 years of research. In a recent review of research since 1992, I summarize the results of various PEMF devices using a range of frequencies and intensities. They have been found to help some of the following conditions: stroke, neuro infections, RSD [reflex sympathetic dystrophy], migraine, muscle sclerosis, spinal degenerative conditions, radiculitis, inguinal nerve injuries, peripheral nerve injuries, Ménière’s, and spinal cord injuries, among others.
Research is even being conducted at the Department of Psychiatry, Harvard Medical School and McLean Hospital. They’re using low intensity PEMFs. Mood improvement was reported by 23 of 30 bipolar disorder subjects who received the PEMF treatment and by four of 14 healthy comparison subjects. Significant differences in mood improvement were found between the bipolar disorder subjects who received actual PEMF stimulation and those who received sham stimulation. The electric fields generated by this low intensity PEMF were smaller (0.7 V/m) than fields used in repetitive transcranial magnetic stimulation (rTMS) treatment of depression (1-500 V/m) and also extended uniformly throughout the head, unlike the highly nonuniform fields used in rTMS. At this point research is ongoing with this system.
Many of the devices listed in our product reviews probably also have significant benefits for mood disorders. Along with this, neurological conditions too. It could possibly help those with psychiatric and neurological conditions.
I’m honored to have been a featured expert in the Proven: Healing Breakthroughs Backed by Science series which details powerful alternative medicines for healing disease. In Episode 6, Overcoming Pain, I outline how PEMFs are effective tools for managing pain by sharing some of the key mechanisms of PEMF therapy. Those mechanisms all have an impact on pain – and more importantly, promote real healing rather than simply masking the pain. I also talk about how well PEMF therapy works with other therapies and modalities to reduce pain and speed recovery.
PEMFs are commonly used to manage chronic back pain and joint pain. This includes pain from arthritis, and pain from other inflammatory conditions. Furthermore, with regular use of PEMFs, you can reduce swelling and inflammation, increase mobility in joints, and find relief from pain. Some research has found magnetic therapy to be more effective than other therapies, such as medications, and as effective as more intensive, expensive therapies like high intensity laser treatments. In addition, once you own a PEMF system, it is available to you to manage a host of other health needs and for health maintenance.
Nonetheless, if you missed this episode – or any other episode in the series, there’s good news. The entire series is available for purchase at a big discount here. That means you haven’t missed a thing! The information is important to anyone looking for safe ways to heal that are backed by scientific research. It has always been my contention that PEMFs do not work alone. They work best when combined with other approaches. These approaches should support the body’s needs and basic levels of function. Nutrition, herbs, and supplements are good examples of what the body has a foundational requirement for. These would be accelerated, activated and enhanced by PEMFs.
When you purchase the series, you’ll have instant access to valuable information from 47 world renowned experts. There are three options to choose from allowing you to select a package that best suits your needs. Each offers lifetime digital access to video, audio and transcripts of all episodes. The silver package includes a digital viewing guide and 2 bonuses. The Gold package includes a paper viewing guide, DVDs, and 2 additional bonuses. The Platinum package is the best value, including everything the Gold package offers along with six additional bonuses. Additionally, you can see the details of each offer here.
Proven: Furthermore, Healing Breakthroughs Backed by Science is your comprehensive source for using alternative and natural therapies for treatment, management, and healing of numerous health conditions, including chronic pain.
In addition, because of the wide, often confusing, array of possible PEMF therapies, drpawluk.com offers opportunities for a no-cost consultation with our medical team to determine the most cost-effective PEMF therapy device for you at: https://www.drpawluk.com/consultation/.
Prostate hyperplasia, also known as benign prostate hyperplasia (BPH), or enlarged prostate, is a fairly common prostate problem for men. In fact, in North America alone, it is one of the most common diseases conditions in men. BPH has several potential dangers and complications for those who suffer from the condition. It can lead to severe discomfort and urinary obstruction, often considered a medical emergency, if severe enough. Not only that, but BPH can also co-occur with prostate cancer. Therefore, it is essential to use BPH treatments that are effective.
The rate of biopsy proven BPH increases from 8 percent in men aged 31-40, to 40-50 percent in men ages 51 to 60, to over 80 percent in men older than age 80. As you can see, benign prostatic hyperplasia is an affliction that is common in older men. In fact, it is so common that most men who are age 50+ will likely develop either BPH symptoms. Benign prostatic hyperplasia (BPH) is a result of urogenital aging. Recent studies suggest that an age-related impairment of the blood supply to the lower urinary tract and chronic inflammation play roles in the development of BPH and thus are contributing factors in the development of BPH.
The prostate gland is normally the size of a walnut and produces prostatic fluid. This fluid is the main component of semen. By the time a man reaches 60 years of age, the swollen prostate may grow to be the size of a lemon. Due to its increased size, it may press more on the bottom of the bladder, causing frequent visits to the bathroom. A common complaint among men who suffer from BPH is that they have to visit the bathroom many times throughout the night.
Although the frequency of urinating is increased, this does not mean that the bladder will completely empty every time. As with most other medical conditions, if BPH is left ignored and untreated it can worsen over time. This can lead to a number of complications.
While BPH is not a life ending condition, it is vital for both patients and doctors to learn as much as they can about how to treat BPH in its early stages. By offering effective enlarged prostate treatment early enough this could prevent the bladder from malfunctioning and potentially harming the kidneys. BPH medications can help stop the condition from developing further.
Medications may slightly reduce swollen prostate size and improve symptoms. However, they have less benefit as the prostate gets larger and prostate health progressively diminishes. A definitive solution for BPH is surgical, or other invasive interventions, to reduce the size of the prostate and improve the flow of urine. BPH has been treated with various types of destructive high energy, high-frequency, radiation methods such as transurethral needle ablation (TUNA), interstitial laser therapy (ILC), and holmium laser resection (HoLRP).
Unfortunately, these therapies often lead to major complications, including urinary incontinence and impotence. Because of the complications of these invasive procedures research shows that men will often try to live with their obstruction symptoms as long as possible.
So, a natural question is whether there are other less risky or dangerous procedures. Or, if there are BPH treatment approaches that can be used that are effective. This is particularly important in the setting of known enlargement without obstruction. This article will explore PEMF therapy and how it can work as an effective BPH treatment for BPH symptoms. We will also discuss some of the recent studies on PEMF for BPH. These are relative in the search for enlarged prostate treatment.
We already understand some of the risk factors and complications that can occur from BPH. However, we do not know as much as is needed. Some of the factors that contribute to BPH are age, prostate infection, inflammation, cardiovascular disease, diabetes, metabolic syndrome and hypertension. It’s likely that multiple risk factors cause BPH.
We have, however, found that inflammatory damage 1 of the most significant factors in the development of BPH. When a man has inflammation, this can trigger a lack of oxygen to the affected area. This inflammation leads to prostate problems and structural prostate and bladder changes. A vicious cycle then develops as the inflammation causes prostate gland remodeling and growth in tissue.
Having said that, age clearly plays an important part in the development of BPH. BPH is a common condition for older men. Some research suggests that a man’s testicles can play a key role, alongside aging. Many doctors even believe that reduced levels of testosterone can occur. While this reduction in testosterone is not contributing to BPH, it can allow dihydrotestosterone to build up, causing the prostate to enlarge. In addition, some further evidence shows that this condition may also be hereditary.
Since there is no cure for BPH, a traditional enlarged prostate treatment for men with BPH includes surgery and medications like alpha-blockers. However, these types of BPH treatments pose potential complications and side effects for the patient. For instance, some of the side effects may include an inability to ejaculate, loss of bladder control, and erectile dysfunction. It can even induce retrograde ejaculation, which is where the semen flows back into the bladder.
Quite clearly, the medical industry needs to develop non-invasive treatments for BPH soon rather than later.
What could PEMF therapy offer patients who are living with BPH and want relief? Is PEMF for BPH a good treatment plan at all? PEMF devices are a non-invasive alternative to help treat many ailments. Pulsed electromagnetic field therapy consists of low frequency waves, that are perfectly harmless to the body. PEMF therapy has been known to help treat many medical conditions including reducing pain.
But how does it work? In simple terms, the electromagnetic energy waves help to reduce inflammation. This then helps to oxygenate the tissues and help blood vessel growth and reduces growth of the excess tissue. Electromagnetic field waves have also been known to help increase a person’s blood flow. Due to a better blood flow, this age-related affliction could potentially be reversed and leading to the prostate pain reducing and decreasing down to normal size.
While we can safely say that PEMF therapy is an ideal non-invasive option, there are few studies relating to PEMF for BPH. These studies set out to determine enlarged prostate treatment for men who suffer from the condition.
However, there have been two published studies where they used PEMF devices to help treat men with BPH and dogs. While these had interesting and variable results, they provide hope for men who are suffering from BPH and seek relief. Continue reading below to find out more about the studies with PEMF for BPH therapy and what it tells us about treating BPH.
Over recent years, there has been some research done to find out how PEMF therapy can help patients who are suffering from various ailments. As PEMF devices have evolved, research has continued to gather data. This is wonderful news for patients and doctors alike as the industry works at finding a solution.
Traditionally, medications have been used to treat BPH. While these medications could reduce the size of the prostate in some men, they do come with their own set of side effects and potential complications. For men who are wanting a non-invasive treatment, the recent studies for PEMF and BHP show great promise.
There have been two therapeutic studies recently that lend support to the use of PEMFs to noninvasively, and safely, reduce the size of the prostate, therefore, increasing prostate health. One of these studies is in humans, the other in dogs.
In the human study, half of the patients with BPH, age 68-78 years old were treated with medication. This lasted for at least 4 weeks. Another group was treated with PEMFs (a high intensity magnetic device, like the PEMF 120) for 2 weeks. This was for for 30 min daily, 5 consecutive days per week. Patients of both groups were evaluated before and after drug and PEMF treatment by values of total PSA, acid phosphatase, ultrasound (U/S) estimation of prostate volume and residual urine, estimation of urine flow rate, and measurement of a subjective International Prostate Symptom Score (IPSS).
There was a significant decrease, before and after treatment, of IPSS and the objective measures of U/S prostate size, residual urine and urine flow rate in the PEMF-treated patients. In contrast, the medication treatment group had only improved the subjective symptom related IPSS. There was also a significant improvement in clinical symptoms in patients of the electromagnetic group. Follow-up of the PEMF treated patients for one year revealed that results obtained by PEMF treatment were still maintained.
The dog prostate is a model for understanding the abnormal growth of the human prostate gland. In a different research study, the authors studied the effectiveness of using PEMFs in dogs to modify prostate blood flow and evaluated its effect on BPH. PEMFs were applied, 5 min, twice a day for 3 weeks, on 20 dogs with BPH. A number of measurements were evaluated before and after treatment: prostate size by ultrasound, semen quality, testosterone levels, plasma volume, composition, and pH.
The PEMF signal (approximately 100 milliTesla – comparable to the Parmeds Ultra) produced a significant reduction in prostatic volume by an average of 57% without any interference with semen quality, or testosterone levels. Doppler ultrasound showed improved circulation. They concluded that this approach would have suitability for the treatment of humans, as seen with the improvement of BPH in dogs, with no side effects. It further supports the theory that impairment of blood supply to the lower urinary tract may be a causative factor in the development of BPH.
Not infrequently, chronic prostate enlargement is caused by a history of infection in the prostate. These infections are notoriously challenging to eradicate. In our book (Magnetic therapy in Eastern Europe: a review of 30 years of research) we reported on one large study evaluating the treatment of chronic prostate inflammation. About 10 to 15 percent of men suffer from this, which can cause disturbances in reproduction and sexual dysfunction.
The cause is unclear and current treatments, especially antibiotics, are largely unsatisfactory. While therapy must be comprehensive, PEMF therapy has been found to be of add-on benefit. A medium intensity (up to 10 mT) pulsed magnetic field device was used with treatments lasting 30 minutes at 25 Hz with exposures to the pelvic perineal area. Some patients were also treated with prostate medication such as antibiotics.
Patients were treated for nine weeks with daily PEMF treatments for the first two weeks, three times per week for the next week, twice per week for two weeks, and then once a week for four weeks. There were statistically significant improvements in pain scores, scores of sexual complaints, and burning on urination. Not only were there subjective improvements but also bladder flow studies improved in five of the six patients with abnormal urine flow curves. Signs of pelvic floor muscle spasm were also reduced.
No changes were found in the laboratory or other tests. There was no change in the PSA. Of the 4 people who did not respond, they had their prostatitis for more than 10 years. Little benefit was typically seen immediately after the treatment course ended. Most of the relief was delayed by up to three months after therapy ended.
Enlargement of the prostate has historically only slightly been accounted for by underlying chronic prostate inflammation. Since prostate enlargement takes place over decades and is, at least in part, related to hormonal influence, any benefit from magnetic therapy in reducing the prostate size would be expected to happen over longer periods of time as well. If there is a significant mechanical obstruction caused by the large prostate, which is not acceptable to live with [and many men do live with this problem] then a surgical or other prostate treatment approach should be attempted.
While the magnetic field therapy may have little direct short-term value on the actual size of the prostate itself, there may be significant benefit in reducing discomfort and possibly improving bladder and urine flow control. Even if surgery and/or other procedures are used, recovery may be helped with PEMF therapy. PEMFs would also help medications, including antibiotics, do their work.
Neurological control of the prostate, bladder and bladder outlet is from the lower spine, therefore PEMFs should be used for this purpose over the lower spine. For bladder control PEMFs can be used over the bladder itself. For perineal discomfort magnets should be placed in this area or sat upon.
Just in case there is concern that PEMFs may increase the risk of any hidden cancers in the prostate gland, another study showed that PEMFs could possibly reduce the growth of prostate cancer cells. Advanced stage hormone resistant prostate cancer currently has a very poor prognosis and no effective therapy. Using human prostate cancer cells, Taxol was added to cell cultures at various concentrations. Also 60 Hz PEMFs from 1 to 5 G were compared. Cell proliferation and cell cycle patterns were assessed. Low dose Taxol was found to inhibit cell proliferation.
After 48 hr of treatment with taxol, prostate cancer cells died. PEMF exposure also induced cancer cell death in human prostate cancer cells. The effect appears to be better when combined with taxol. So, Taxol and 60 Hz PEMFs appeared to induce prostate cancer cells to die. These encouraging results suggest an alternative anti-cancer effect of taxol and 60 Hz PEMF exposure on human prostate cancer cells. Effects of 60 Hz PEMFs on human prostate cancer cells demonstrate potential clinical therapeutic effects of PEMFs.
So, to conclude, PEMF therapies appear to be a promising approach to help manage a challenging health condition. BPH is a very common condition in men, particularly as they get older. What we do know is that, as with most medical conditions, the earlier treatment is used, the more chance of not suffering complications. If enlarged prostate treatment is offered sooner than later, this is likely to help the man prevent swelling and urinary obstruction.
This is especially important given that the current alternative therapy tends to be more invasive with the risk of side effects and for which current medical management is not very helpful in the long run, and rarely prevents progression of the condition. Some complications from invasive treatment can leave the patient feeling frustrated and dramatically affect quality of life. It is quite likely that PEMF treatment will have to be long-term in order to achieve the best results and prevent the problem from returning. It also appears that higher intensity PEMFs are necessary to achieve the results found in the two studies cited above and to reduce chronic inflammation.
Effects of pulsed electromagnetic fields on benign prostate hyperplasia. Giannakopoulos XK, Giotis C, Karkabounas SCh, Verginadis II, Simos YV, Peschos D, Evangelou AM. Int Urol Nephrol. 2011 Dec;43(4):955-60.
Effect of pulsed electromagnetic field therapy on prostate volume and vascularity in the treatment of benign prostatic hyperplasia: A pilot study in a canine model. Leoci R, Aiudi G, Silvestre F, Lissner E, Lacalandra GM. Prostate. 2014 Aug;74(11):1132-41.
Potential clinical application of taxol and power frequency electromagnetic fields exposure on human prostate disorders. Ning, J. T.; Gajendran, V.; Porter, C.; Medica, J.; Stein, B. S.; Zabbo, A.; Cohen, S. I.; Czerska, E. M.; Casamento, J. Second World Congress for Electricity and Magnetism in Biology and Medicine, 8-13 June, Bologna, Italy, Abstract No. I-7, p. 136-137.
Pain following amputations (post-amputation pain – PAP) is very common and challenging to treat. There are many mechanisms that cause PAP. They involve brain, spinal and local aspects. The brain aspects involve reorganization of brain nerve patterns representing the amputated limb that result in phantom limb pain (PLP) and phantom sensations (PS). There can also be reorganization of spinal nerve patterns with the peripheral nerve injury associated with the amputation. In the stump area nerve damage causes inflammation, regenerative nerve sprouting, and increased nerve signals in the remaining limb or the development of a neuroma.
Treatment should be individualized. Treatments mostly include injection therapy, medications, alternative therapies, surgery, and prevention strategies. Treatments can be targeted to the brain, spinal cord or locally to the stump. Pulsed electromagnetic field (PEMF) therapy is a safe, low risk, noninvasive, externally applied therapy that has been found to be effective in helping PAP and PLP. This therapy may even be applied daily in the home setting for the best long-term results.
There is archaeological evidence for intentional amputations dating back at least 45,000 years. Major advancements in the care of amputations have happened as result of improvements in dealing with injuries from wars over the centuries. Weir Mitchell coined the term “phantom pain” when reporting on 86 Civil War amputees, where 90% had PLP. (Louis; Mitchell) PAP is considered one of the most challenging of all pain conditions to treat. After all, how can you treat a phantom? It is now recognized that the challenge stems from the fact that there are many physical mechanisms that lead to PLP.
In the US, in 2005 1.6 million people lost limbs. This is projected to increase to 3.6 million by 2050. (Hsu)
about 185,000 amputations are done every year. Vascular disease is the most common cause at 82%, followed by trauma [16%], cancer [0.9%] and congenital anomalies [0.8%]. At least 95% of those with limb loss experience PLP, PS or residual limb pain (RLP). Amputees have a hard time distinguishing between these different forms.
PLP is a painful or unpleasant sensation in the lost body part – the part that no longer exists. PLP can be felt as sharp, shooting or electrical lakes sensations or dull, squeezing, or cramping pain. It can be felt in the entire limb or just one area of the limb. PLP typically shows up within the first 6 months after amputation. By the time several years passes, about 85% can have PLP and can persist for years. PLP can change over time from a knife like/sticking sensation involving the entire missing limb to a burning/squeezing sensation in the further areas of the missing limb.
Published PLP rates range from 50% to 80% of limb amputees, with 5–10% of these individuals experiencing extreme pain (Batsford; Yin). Variations in prevalence are based on pre-amputation pain, amputation location, anesthetic and surgical procedure, sex, psychological factors, and time after amputation (Richardson; Aiyer). Almost immediately following the amputation of a limb, 90–98% of patients report experiencing a phantom sensation.
Nearly 75% of individuals experience the phantom as soon as anesthesia wears off, and the remaining 25% of patients experience phantoms within a few days or weeks. Literature indicates that majority of amputees suffer PLP in the year following their amputation, but with time declines from 72% at 8 days, 65% at 6 months and 59% at 2 years (Collins). Likewise, there are lower prevalence rates of phantom pain over time, 32% at 6 months, 26% at 1 year and a half, 23% at 2 years and a half and 27% at 3 years and a half after amputation (Bosmans).
RLP or “stump pain” is often felt as sharp, burning, electrical like or “skin-sensitive” pain in the incision, felt deep in the remaining limb or sometimes involve the whole remaining limb. Stump pain can happen about 74% of the time and like PLP can persist for years. The stump pain may be classified into multiple categories depending on cause. Stump pain is usually more bothersome right after amputation, with PLP becoming more dominant 1 – 12 months afterwards. There’s a big correlation between severity RLP and PLP.
PSs are nonpainful perceptions coming from the lost body part. They are common after the surgery. One third have sensations within 24 hours, three quarters within 4 days and 90% within 6 months. PSs can also happen after nerve injuries or spinal cord injuries without amputations. They can be sensed as movements of the amputated part that can be willed or spontaneous. There can be sensations related to the size, shape or position of the missing part, such as feeling that a foot is twisted.
There may also be sensations of touch, pressure, tingling, temperature, itching or vibration. They are more likely to involve sensations relating to the hands or feet. PSs can also occur from loss of other body parts, including about 25% of those with mastectomies. Another sensation is the sense of shortening of the amputated limb, so that it doesn’t feel the same in size or length. This is called telescoping and happens in one quarter to two-thirds of amputees.
PLP is further complicated by pre-existing orthopedic issues, such as low back pain from disk or spine problems, vascular insufficiency problems above the level of the body part being amputated, among others. PLP or stump pain may be related to a local neuroma in the stump or even to prosthesis-related pain. The latter happens especially over time as the stump changes shape and size and a prosthesis needs to be remolded or readjusted. Bone or graft infections are not uncommon as well.
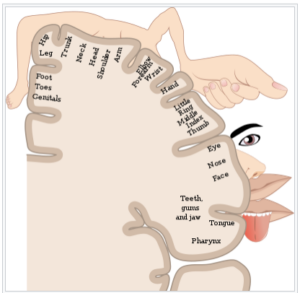
All the different parts of the body are represented by sensory nerves, grouped by area into “maps,” called homunuculi, that relate to the density of sensory neurons in a given body area. This image is one example of a cortical sensory map.
From: https://en.wikipedia.org/wiki/Cortical_homunculus
Brain related causes of PLP are due to reorganization of the nerve pathways in the somatosensory cortex of the brain surrounding the area that would normally represent the lost limb. For example, brushing the face of upper limb amputees can elicit PSs, because these areas are close to the area represented by the lost limb. Therefore, there would be spillover of sensory information into the area that still contains neurons representing the lost limb.
The neurons are still there but there is no sensory information coming to them from a lost limb. Brain imaging studies show that the area representing a lost hand is activated during movement of the remaining arm. In fact, stimulation of the brain in the brain area representing the lost limb can cause contraction of the rest of the extremity. The greater the size of the brain area of the lost sensation the more intense the PSs.
Sources of PLP from the stump can be from spontaneous nerve activity from the cut end of nerves. If this is the source of the PLP/stump pain, injection of local anesthetic will often give temporary relief. This spontaneous activity of the nerves in the stump can lead to the pain being made worse or initiated by emotional distress, exposure to cold, and other stimuli.
Spinal sources for PHP/PLP happen because of decreased nerve traffic into the spinal cord. With decreased nerve traffic into the spinal cord, the brainstem does not send down the normal inhibitory messages to decrease whatever sensory traffic remains. This situation can end up creating autonomous firing of spinal neurons, effectively becoming “sensory epileptic discharges” in the spinal cord. This is essentially “spinal reorganization”, comparable to cortical reorganization. Spinal reorganization is seen in lower limb amputees who develop new disc herniations or shingles infections.
There are many other spinal and brainstem changes that happen over time, including neuronal atrophy, that make the post amputation physical changes complex. As an example, even spinal anesthesia can rekindle previously inactive PLP.
Treatments conventionally include spinal reorganization injections, medications, alternative therapies, surgery and attempts at prevention. Local injections, including anesthetics or botulinum, are more useful in RLP or stump pain and often give little sustainable help for PLP.
Medications are variably helpful, may create addiction, immune challenges and other side effects. They rarely cure the problem, which can recur when the medication is stopped. Because PAP treatments are so challenging and have limited benefits, alternative therapies have been used frequently. Some include psychological therapy, cognitive behavioral therapy, hypnosis, etc., there is little evidence for long-term benefit. Mirror therapy has gained popularity and can have short-term benefits with improved pain scores. However, there is no evidence for long-term benefits.
Surgical therapies, especially peripheral nerve reconstruction, have mixed results, can have significant complications and side effects and should only be considered as a last resort, with the failure of other less invasive approaches, including neuromodulation.
Prevention approaches have been used preoperatively, during surgery or within 2 weeks of the amputation. Some of these approaches have included epidural injections, regional nerve blocks, infusions and TENS. Long-term benefits have been limited, and one review found that there was limited evidence of benefit for treatments in the acute postoperative period. Results have been inconsistent and variable, especially for longer-term benefits.
Amputation not only results in the loss of neural input/feedback from the amputated limb but also produces a loss of visual and tactile information related to the limb. The brain influences that normally inhibit pain may be further reduced by the absence of information from these external sources that might otherwise confirm or reduce the perception of pain arising from the periphery (for example, a phantom limb in a painful position or a “crawling” sensation on the skin). Thus, some forms of PLP may arise, in part, from a release from inhibitory control (that is, disinhibition).
Mirror therapy (MT) is a long-standing treatment for PLP and is to work by restoring normal somatosensory and visual inputs to the brain. (Aternali) Individuals were instructed to move both the intact and phantom limb at the same time during MT while viewing the reflected image of the intact limb in the mirror in the place of where the amputated limb would have been.
A recent neuroimaging study of lower limb amputees with PLP found that viewing mirror images of feet (but not hands) in the foot area of sensorimotor cortex of the brain opposite to the amputated limb as well as in posterior parietal cortex produced better results. Unfortunately, the intensity of the PLP and the increased visual responsiveness no longer worked after 4 weeks of MT. Seeing the limb (via MT) re-establishes the normal inhibitory sensation control processes.
MT restores inhibitory control over brain cells receiving sensory information in these and other brain regions and reduces abnormal brain activity, which contribute to the PLP, and thereby reduces pain. The results of the most recent studies evaluating the efficacy of MT for PLP are not promising, especially long-term. Overall, MT does not appear to reduce PLP to a greater degree than control or other known treatments. At least, it’s inexpensive.
PEMF treatment can be applied to the stump, the spine or the brain. For the treatment of the PLP itself, there is almost no research using lower intensity PEMF systems. There is significant evidence for the value of PEMFs in dealing with chronic pain in general, whether treating the brain or periphery. (Pawluk, 2015) PEMFs are also established for helping wound healing (Pawluk, 2017)
There is some research on the value of transcranial magnetic stimulation (TMS) for PLP.
One group (Nardone) did a systematic review using PEMFs in individuals with PLP and PS. Brain imaging found an enlarged increased cortical excitability in the opposite hemisphere to the PLP. However, these cortical excitability changes and PLP do not correlate with each other. TMS influences brain function when used repetitively. TMS to the opposite brain area led to a transient reduction in pain intensity. Stimulation can be to the opposite motor cortex. The natural, endogenous painkilling chemical, Beta-endorphin, increases significantly after stimulation to the opposite motor cortex.
Another clinical review (García-Pallero) also found that TMS was effective in decreasing pain in PLP and symptoms of anxiety and depression compared to simulated TMS or placebo. Pain syndromes other than PLP can be improved by TMS. Stimulation of the opposite parietal cortex decreased pain intensity of up to 10 minutes, with no clear effect on pain in other cortical areas. Even stimuli used for 3 consecutive weeks on the opposite parietal cortex did not result in lasting improvements. PLP in the parietal cortex is due to dysfunctional activity. In 27 patients with PLP after unilateral amputation, 5 consecutive days of 10 minutes of real TMS over the hand region of motor cortex every day versus sham stimulation, VAS (Visual Analogue Scale) and LANSS scores (Leeds Assessment of Neuropathic Symptoms and Signs) decreased significantly.
Depression and anxiety levels decreased significantly. Finally, beta-endorphin was assessed 1 to 2 hours after five sessions and significantly increased after real stimulation. In TMS treatment of PLP in landmine victims, of 49 individuals, 26 of whom received real TMS over the opposite side brain motor strip (M1), there was no significant overall average visual analog pain scale (VAS) differences at 15 or 30 days. However, a decrease in VAS was seen by more than 30% of the individuals at both 15 days and 30 days.
Another clinical trial found that TMS caused significantly better pain relief 15 days after active treatment versus placebo stimulation. But this benefit was gone 30 days after treatment. 70% of those in the active group had clinically significant pain relief (> 30% relief), compared to 41% in the sham group. In this study, anxiety and depression symptoms weren’t different. This trial again points out the need for longer-term PEMF treatment.
As stated earlier, PAP or PLP may be affected by spinal cord functional signal traffic disinhibition, even without spinal cord injury, suggesting a possible benefit from spinal cord treatment. PEMFs have been found to have significant regenerative effects on spinal cord injuries and function. (Ross; Kumar) PEMFs can indirectly electrically activate spinal circuits with the noninvasive pulsed electromagnetic field (PEMF) applied over intact vertebrae, safely passing through the tissues to reach the spinal cord. So, when direct brain stimulation or direct stump stimulation doesn’t work to reduce PAP or PLP, spinal cord stimulation can be attempted or added. This should also be considered when the benefits from direct brain stimulation or stump stimulation are less than optimal.
Phase 1. Moderate to high intensity PEMF therapy to the stump. The researched therapy with the best noninvasive therapy results for PLP is high intensity transcranial brain stimulation. Since stump pain is the easiest to access and a common cause of not only local pain but also phantom limb pain, treatment of the stump as an initial strategy may be simplest and easiest. For this purpose, moderate to high intensity PEMF therapy daily in the home setting may be best strategy, especially if started as soon after amputation as possible. In this case local PEMF therapy may prevent the onset of phantom limb pain, which often does not start for some time after the amputation.
If this resolves the local pain and/or phantom limb pain, exploring other approaches may not be necessary. As commonly happens, early results can be short-lived, especially if therapy is not continued. In this case it may be best to do local therapy for several months, even after the pain has been resolved, so that imperceptible, deep tissue healing, especially of nerves, can still produce results. A local, portable PEMF device may work well to a stump and can be used for hours at a time daily. Higher intensity PEMF devices can be combined with lower intensity portable equipment for better and faster results.
Phase 2. High intensity transcranial brain stimulation. While local pain problems may be resolved naturally or with physical therapy, after amputation, phantom limb pain may still begin at any time without any contribution from the stump. If that happens, the next phase of therapy should be transcranial stimulation. For this purpose, high intensity PEMF, done daily for a minimum of 30 minutes twice a day, whether it’s to the opposite side of the brain to the amputation or the same side, doesn’t matter and will be a matter of trial and error for which works best.
While not researched, it may be possible to alternate sides of the brain on the same day of treatment. Treatment should be continued until the pain is resolved. If treatment is stopped and the pain returns, then treatment should be started again. It is hoped that, if this happens, re-starting treatment may produce results faster. Phantom limb pain or phantom sensations may continue indefinitely, hopefully lessened by PEMF therapy, which is the rationale for owning a home-based PEMF therapy system. Getting the assistance of a PEMF expert may be best to achieve the best results.
Phase 3. High intensity spinal stimulation. If treatment is not either fully or partially successful with local and/or transcranial PEMF treatment, treating the spine may be considered next. This may be done at the back of the neck, mid back or the lower back. Trial and error may give the best indication for which treatment area produces the best results. As with the other therapies, treatment may need to be at least twice a day for months before a conclusion can be reached about the effectiveness. As with other therapies, initial results may not continue, so treatment may have to be reinitiated again for some interval. This may happen multiple times.
Phase 4. High intensity stump, brain (transcranial) and spinal stimulation.
It’s possible that after all the above approaches have been tried individually with less-than-optimal results, it may be necessary to treat 2 or 3 different areas (local, brain and/or spinal cord) either at the same treatment session or during the same day. This will need to be a matter of trial and error.
Because PEMF therapy stimulates tissues to heal, initial reactions, such as increased pain, are common and resolve with continued treatment as healing of the tissue, reduction in nerve irritability and cortical excitability are facilitated. Nevertheless, it may be necessary to start off with lower intensities and shorter treatment times, which then can be gradually increased as symptoms improve, and healing occurs. Examples of going low and slow are available in the blog section on DrPawluk.com.
Assistance with PEMF therapy, whether for purchase of a device or ongoing therapy support, can be obtained through DrPawluk.com. Another good resource for general support for PEMF therapy can be obtained through the book Supercharge Your Health with PEMF therapy.
Persistent pain following amputation is very common. It is also very frustrating to treat with limited benefits and minimal risk. There are 3 types of persistent pain, stump pain, phantom limb pain and pain initiated or maintained by spinal cord processes. Phantom limb pain is most commonly and most effectively managed by neuromodulation of the brain, using pulsed electromagnetic field therapy. PEMFs can be obtained and used in each of the common settings of post amputation pain. There will need to be some significant trial and error to determine the best protocols for any given individual. It is very likely that treatment will need to be continued for extended periods of time, even perhaps indefinitely.
There’s a lot of confusion around the differences with Pulsed Electromagnetic Field (PEMF) devices. Most often with other electrotherapy and electrical stimulation (e-stim) devices. This is especially true for Transcutaneous Electrical Nerve Stimulation (TENS) machines. Although there are some similarities, there are also some very big differences in PEMF vs. TENS – particularly in the way each is applied and how this impacts the way they interact with the body.
TENS units use electric currents while PEMF devices use pulsed electromagnetic fields. PEMFs have effects on the brain and at the cellular level in your body. They don’t simply stimulating nerve activity. This means that PEMFs offer deeper healing as well as the pain management effects TENS units provide.
The purpose of TENS units are to help patients manage pain. They work by a distraction technique, called the gate control theory. Basically, TENS operates by confusing the brain through the stimulation signals it produces. It competes with the signals from another pain source. So, TENS stimulation is like stomping on your big toe when you have a headache. The pain in the toe now is stronger than the headache pain. Thus, it overshadows the headache. This is usually a very temporary benefit.
PEMFs are designed to stimulate repair of tissues at the cellular level. Repair and healing of the cause of the pain is what produces longer-lasting pain relief. TENS is mostly used for pain. However, it does so mostly without healing the cause of the pain. In addition to giving pain relief, PEMFs have a whole range of other health care applications. Research has shown that PEMFs can stimulate healing for wounds and bone fractures. They can also have a positive impact on depression and anxiety. Furthermore they improve sleep quality, and many more benefits beyond pain relief.
PEMFs work at the mitochondrial level to repair cells and tissues. TENS stimulates nerves and activates the opioid system, changing perception of pain. Therefore, TENS units don’t impact actual healing – they simply manage the pain of the injury.
PEMFs do that, and more! PEMF therapy is also highly effective in the repair of damaged cells. Along with this, it benefits neuron stimulation, calming inflammation, and helping to create new cells. Since a PEMF device can also manage pain, there are a lot of good reasons to choose PEMF therapy over TENS therapy.
Beyond the actual therapeutic benefits PEMFs offer, convenience is another factor that makes them a more appealing option. TENS units must have direct skin contact, making them more difficult to use. PEMFs, however, can be used over light clothing. This allows for use in more settings – such as sitting in your chair in a cubicle, or even while you’re driving.
Because PEMF devices come in a range of unique delivery options – such as a chair pad, total body pad, or smaller rings and paddles, they can target more of the body at once than TENS units can. With a TENS unit, electrodes must be moved from one spot to another on the body, which can take more time and effort to accomplish.
As I’ve said already, PEMF devices have a wide range of therapeutic benefits, far beyond the pain management function of TENS units. Some of these additional benefits might be surprising, but the reach of PEMF therapy is a lot wider than you might think. Insomnia, cancer management, and weight loss are some of the unique conditions that PEMFs can help, which TENS units cannot.
One result that you might not expect to gain from PEMF therapy has been discovered in the research: PEMF therapy is effective treatment for a range of sleep issues, including insomnia! A double blind study in 2012 found that 90% of participants with insomnia felt relief within just four weeks – and 75% no longer suffered from insomnia at all!
Since sleep is such an important aspect of the healing process, and enhances cellular regeneration, this is a tremendous added benefit. It’s easy, effective and convenient. And not only are sleep disorders resolved, the underlying cause (most often depression) can also be healed – which means the sleep issues may not return later.
Cancer treatments often bring a range of unpleasant side effects and low rates of total remission. New therapeutic strategies are essential, and the use of PEMF therapy in cancer treatment offers many potential benefits.
PEMF therapy is non-invasive, safe, and will not be toxic to non-cancerous cells like so many traditional cancer treatments are. PEMF therapy has been tested in cellular and animal applications, and so far in very limited application in human cancer. Although much more research is necessary, initial findings suggest that PEMF therapy, especially in combination with other treatments, can offer real benefits in the treatment of cancer.
In vitro (outside of living organisms) research has found that PEMFs inhibit growth of cancerous cells and reduce tumor growth, among other findings. In vivo (within a living organism) research supports the claim that, when compared to untreated control groups, all treated groups show slower rate of tumor growth.
Two clinical studies using PEMF therapy for cancer treatment showed that, compared to other cancer treatments, PEMF therapy is a safe and promising alternative.
Weight loss and fat reduction are also areas that can be positively impacted by PEMF therapy. PEMF therapy, through its direct cell stimulation, creates more energy, which in turn boots metabolism.
Release of fatty acids from fat cells and improved circulation are additional ways that PEMF therapy can help with weight loss. With better circulation, stubborn fat deposits can be mobilized and get to the bloodstream, where they can be used as energy for the body.
Weight loss is also greatly impacted by the reward centers in the brain, as well as the bacteria in the gut. PEMF therapy stimulates the reward centers, reducing cravings, and helps change the balance of bacteria to a more beneficial state, thus aiding in weight loss.
In addition to all those added benefits that PEMF therapy offers as compared to the primary pain management function accomplished by TENS therapy, PEMF devices offer an impeccable record of safety and are a much better investment due to the range of capabilities a unit offers.
Animal research has shown that stimulation above 20 Hz can have negative side effects. TENS units are often set to >50Hz, meaning they can only be used sparingly – 30 to 60 minutes a day, short term only.
PEMFs, on the other hand, are often set below 20 Hz – typically even under 10 Hz. This low frequency treatment can be used for extended periods of time, multiple times per day if desired. Some systems can even be run overnight, promoting healthy sleep and healing without disrupting any part of your day.
Properly applied PEMFs have shown no adverse side effects – unlike many conventional treatments for pain and other conditions. Because PEMFs always pass all the way through the body, there’s no danger of overdose as there is with pain medications.
A TENS unit has very specific applications, which means your investment might sit on a shelf more often that it’s in use. PEMFs, however, can be used to treat so many health problems – and are also very beneficial as preventative care. So when you invest in one, you (and your whole family) can reap multiple benefits This is true even after the condition you initially purchased the unit to treat has been resolved.
To reiterate the comparisons between PEMF therapy and TENS therapy, while they are similar in some ways, there are many reasons why PEMF therapy is the right way to go. PEMF devices are more convenient, as they don’t require direct skin contact, like TENS. The coils can be put over clothing, and even under shoes. PEMF devices can be used more often. They’re for a wide range of health concerns that extends well beyond pain management. PEMF devices have a solid reputation for safety, with no adverse side effects.
Get guidance in selecting a PEMF device. Call our office to speak with a member of our team at (866) 455-7688. We can help you find the product that best suits your health needs and budget.
Pelka R, Jaenicke C, Gruenwald J. Impulse magnetic-field therapy for insomnia: a double-blind, placebo-controlled study. Adv Ther. 2001;18(4):174-180. [PubMed]
Vadalà, M., Morales-Medina, J. C., Vallelunga, A., Palmieri, B., Laurino, C., & Iannitti, T. (). Mechanisms and therapeutic effectiveness of pulsed electromagnetic field therapy in oncology. Cancer medicine, 5(11), 3128–3139. doi:10.1002/cam4.861